CNT Validity Indicators
Overview
The 8 tests on the CNT generate a number of “validity indicators” (VI). These are tests within tests, embedded in the test battery to discover whether a patient has put forth an appropriate level of effort. In the presence of a completed test battery, a high number of negative validity indicators is strongly suggestive that the patient’s low level of performance is motivational in nature, rather than psychological, physical or neuropsychiatric.
The VI were determined in studies comparing patients with various traumatic brain injuries to suspected malingerers (SM) and to people who were pretending to malinger a brain injury (DMAL). The two malingering groups scored much lower on all the tests compared to brain injury patients.
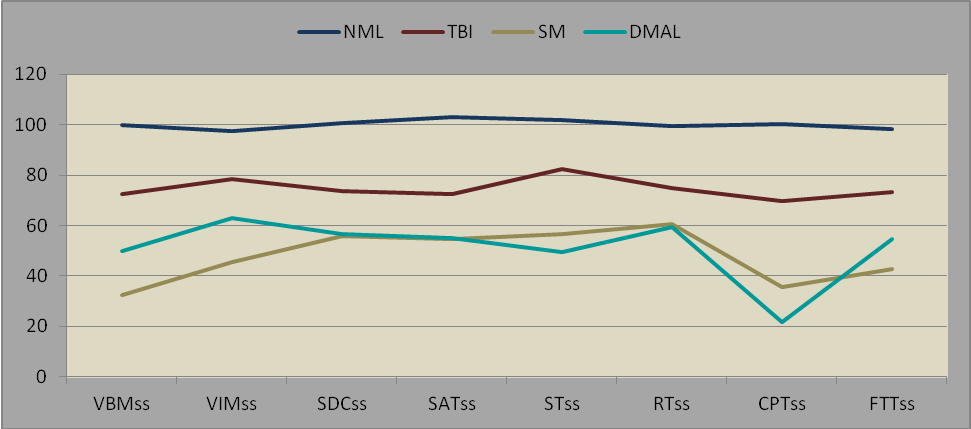
INDEX SCORES OF NORMALS, TBI PATIENTS AND 2 GROUPS OF MALINGERERS
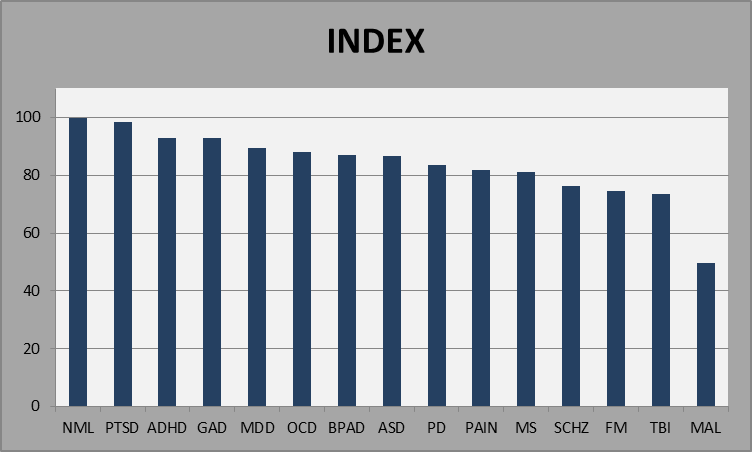
INDEX SCORES OF PATIENTS WITH VARIOUS DIAGNOSES AND MALINGERERS
VALIDITY INDICATOR 1: INDEX SCORE LESS THAN 45
If the Index score is less than 45 the probability of an invalid test is 90%. In our database, there were no normal subjects who scored less than 45; only 10% of severe TBI patients did; but 45% of malingerers did. Even patients with mild dementia and mild mental retardation will usually score higher than 45.
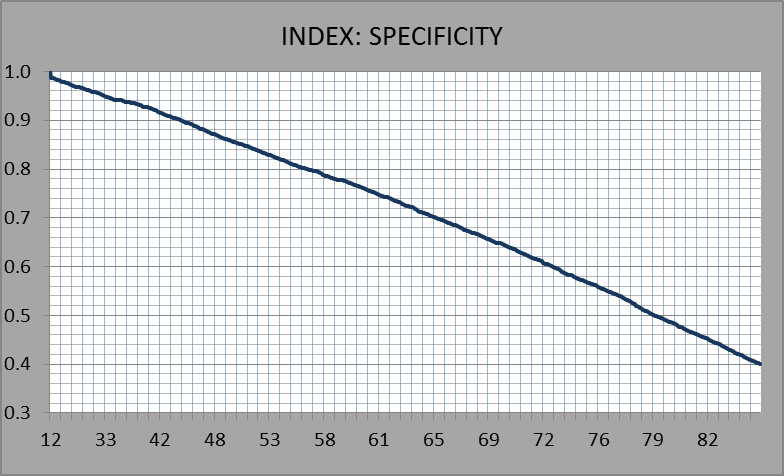
FIGURE 2.6.1.1 INDEX SCORE BELOW 45
VALIDITY INDICATOR 2: TESTS THAT ARE FORCED-CHOICE TESTS.
The verbal and visual memory tests in CNT are recognition memory tests. In each test, there are 60 items and to each item the participant is asked to respond yes, if the item is correct or no if the item is incorrect. The VBM and VIM also happen to be forced choice tests; that is, pressing the button every time, or not pressing the button at all, should generate a test score of 30±3 on VBM or VIM. Theoretically, a score less than 30 on VBM or VM indicates willful exaggeration. Someone who simply presses the button randomly, or does not press the button at all, ought to score 30. Therefore, a score less than 30 is, ipso facto, is not only an invalid response, but one suggestive of willful manipulation.
On the VBM and VIM, raw scores less than 34 indicate invalid responding; that is, responding that is random. Scores below 30 are suggestive of willful exaggeration. In a recent study, we found that none of the 2172 normal participants scored less than 30 on VBM or VIM. Among 589 severe TBI patients, 14 (2%) scored below 30 on VBM (n=6) or VIM (n=8). In contrast, among the 40 individuals in a group of suspected malingerers, 17 scored below 30 on the VBM or the VIM and two scored below 30 on both. In a group of 60 “directed malingerers,” that is, normal subjects who were instructed to behave as if they had severe brain injuries, 17 scored below 30 on VBM or VIM and 9 scored below 30 on both.
The Shifting Attention Test is also a forced choice test. One has to match the target by shape or color. If a subject makes more errors on this test than correct responses, it may also be a sign of willful exaggeration. Few if any normal subjects make more errors than correct responses; in our study, 27% of severe TBI patients did and 60% of malingerers.
NUMBER OF TEST SCORES LESS THAN 70.
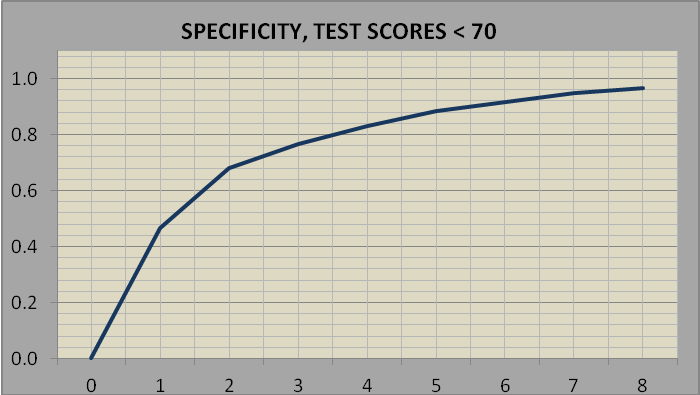
It’s not unusual for someone to score less than 70 (standard score) on a particular test. It is unusual for someone to score below 70 on 3 tests (80% likelihood of test invalidity) or on 5 tests (90% likelihood). Count up the number of standard scores below 70 on the nine summary test scores on page 1 of the report.
NUMBER OF TEST SCORES BELOW 70
Note, Figure 3: x axis, number of test scores < 70; y axis, probability of noncredible responding
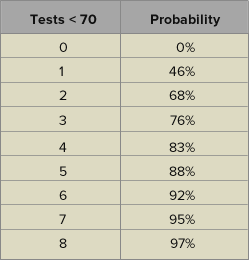
PROBABILITY OF NON-CREDIBLE RESPONSE PATTERN BY NUMBER OF TEST SCORES LESS THAN 70
TEST VALIDITY INDICATORS BASED ON RAW SCORES.
The method was to generate an ROC curve based on malingerers vs. TBI patients and select a cut point with ~40% sensitivity and ~90% specificity. We made adjustments to the cut point numbers in order to allow the examiner to score the test without recourse to tables or to the computer program, and also to recognize the particular qualities of the test, for example, a negative Stroop effect (incongruent response time faster than congruent response time), and more errors than correct responses on the shifting attention test.
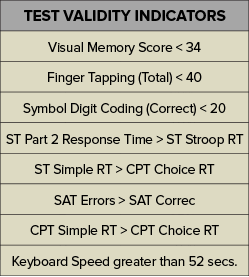
TABLE 2.6.4.1. VALIDITY INDICATORS ON THE INDIVIDUAL TESTS
MALINGERERS’ PATTERN OF RESPONSE ON REACTION TIME MEASURES.
Malingerers are extremely slow in tests of simple reaction time and relatively faster in measures of choice or complex reaction time. Thew figure below identifies two reaction time measures: 1) Simple Reaction Time (SRT), the average of the simple reaction time scores from the first parts of the Stroop test and the working memory test, and 2) Choice Reaction Time (CRT), the average of the choice reaction time tests in the CPT and part 2 of the working memory test. The two groups of malingerers were the only groups whose SRT scores were longer than their CRT scores.
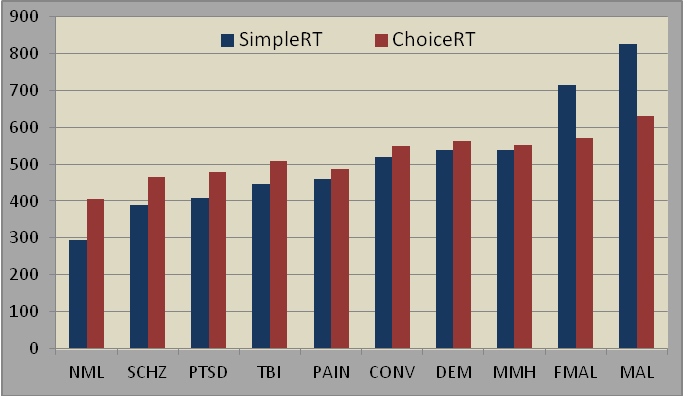
SIMPLE AND CHOICE REACTION TIMES
Note: FMAL = directed malingerers; MAL = suspected malingerers
CONVERSION DISORDER COMPARED TO MALINGERERS.
It’s not always easy to distinguish between someone with a somatoform disorder and a malingerer, but on the CNT there are clear differences. Conversion disorder patients seldom if ever score below 30 on the VBM or VIM. As a rule, CD patients do poorly on the CNT, about as bad as a severe TBI patient or a chronic pain patient but not nearly so bad as a malingerer.
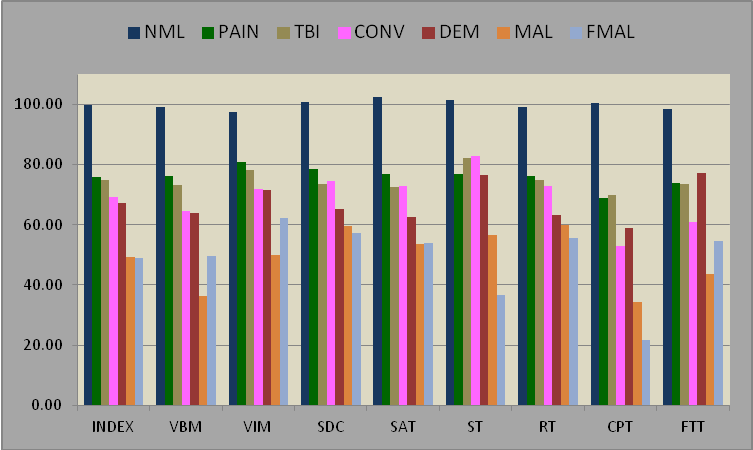
CONVERSION DISORDER PATIENTS COMPARED TO SIX OTHER GROUPS